by Marcos E. Fernández-Cuadros 1,2,*,Olga S. Pérez-Moro 1,2,María J. Albaladejo-Florín 1,2,María M. Tobar-Izquierdo 2,3,Amelia Magaña-Sánchez 2,3,Patricia Jiménez-Cuevas 2,3 andJavier Rodríguez-de-Cía 2,3
1Servicio de Rehabilitación y Medicina Física, Hospital Universitario Santa Cristina, 28009 Madrid, Spain
2Instituto de Investigación Sanitaria del Hospital Universitario la Princesa, 28009 Madrid, Spain
3Servicio de Análisis Clínicos, Hospital Universitario Santa Cristina, 28009 Madrid, Spain
Academic Editor: Gregorio Martínez Sánchez
Processes2022, 10(1), 138; https://doi.org/10.3390/pr10010138Received: 19 November 2021 / Revised: 4 January 2022 / Accepted: 7 January 2022 / Published: 10 January 2022(This article belongs to the Special Issue Basic, Biological and Therapeutic Processes of Ozone Therapy)
Abstract
Objectives: (1) to demonstrate the anti-inflammatory and anabolic effect of Ozone by determining in serum samples the biochemical levels of IL-6 and IGF-1 in knee osteoarthritis (OA) patients in a real world rehabilitation setting; (2) to differentiate Ozone effect in diabetic (DM)/obese and non-DM/non-obese patients; (3) to evaluate clinical effectiveness by visual analog scale (VAS) and WOMAC scale, and biochemical effect by C-reactive protein (CRP), uric acid and erythrocyte sedimentation rate (ESR). Material and methods: 65 patients with knee OA Kellgren Lawrence (KL) grade 2 or more were analyzed in a retrospective observational study. The study ran from January 2018 to September 2021. Inclusion criteria: (a) patients 18 years or older; (b) with knee OA KL 2° or more; (c) biochemical analysis before-and-after treatment; (d) pain more than 3 on VAS. Exclusion Criteria: (a) previous knee surgery; (b) favism; (c) pregnancy; (d) any other disease that originates lack of collaboration for infiltration. Primary Outcome variables: (a) IL-6; (b) IGF-1 in diabetes mellitus (DM)/obese and non-DM/non-obese patients; both before-and-after Ozone treatment. Secondary Outcome variables: (a) CRP, (b) ESR, (c) uric acid, (d) VAS pain, (e) WOMAC pain, function and stiffness. Ozone protocol consisted of four sessions (once a week) of an intra-articular infiltration of 20 mL (20 µg/mL concentration) of a gas mixture of Oxygen-Ozone 95-5% (produced by Ozone generator Ozonosan-α Plus®). For biochemical evaluation, SNIBE MAGLUMI ™ IL-6 (CLIA) and SNIBE MAGLUMI ™ IGF-1 (CLIA) kits were used. CRP and uric acid were analyzed by a Abbott Alinity c kit; and ESR was evaluated by DIESSE VES MATIC CUBE 30. Results: There is a linear correlation between age and OA severity. IL-6 decreased both in DM and non-DM patients and in all OA KL grades (from 2.70 to 1.59 pg/mL). IGF-1 decreased in total group (OA + DM + obesity) from 112.09 to 107.19 ng/mL. When only non-DM/non-obese knee OA patients were analyzed, Ozone improved IGF-1 levels (from 100.17 to 102.03 ng/mL). Ozone decreased CRP, ESR, uric acid, and improved VAS pain, WOMAC pain, function and stiffness (p < 0.05).
Conclusions: Ozone is a valid option for the management of knee osteoarthritis in a real world rehabilitation setting, because of its anti-inflammatory, metabolic and anabolic properties. Ozone tends to downregulate pro-inflammatory IL-6 cytokine. Ozone has a metabolic/hypoglycemic effect on obese/diabetic knee osteoarthritis patients by reducing IGF-1. Ozone has an anabolic effect on non-diabetic/non-obese patients by improving IGF-1. Ozone reduces other biomarkers of inflammation (CRP, ESR and uric acid) and improves, pain, function and quality of life.
1. Introduction
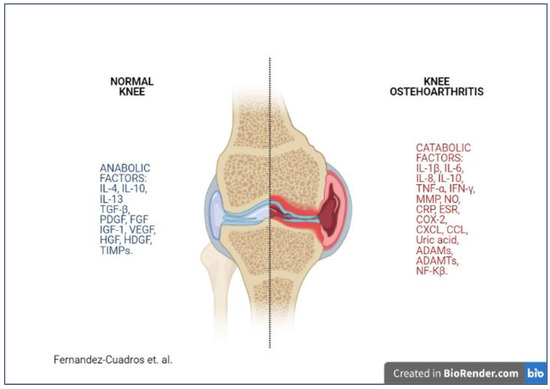
Osteoarthritis (OA) is the most common source of arthritis. OA affects the quality of life to an extent that it is the 11th contributor of global disability worldwide. In Spain, OA burden is such that at least four million people are affected and 4378 million € per year are direct cost, which represent almost 0.5% of the Gross Domestic Product [1].OA is so prevalent that in people over 50 years of age, 70% of them have at least one radiological sign in some articulation; in people over 60 years of age, 13% of them refer to OA pain in their knee; in those over 70 years of age, 27% have radiological signs; and in people over 80 years of age, 44% show clinical symptoms and radiological signs [2].Knee OA is the most common type of OA. Cartilage breakdown, bone degeneration and narrowing of articular space are typical signs. Knee OA is multifactorial, mechanical and inflammatory factors attributed to OA pathophysiology [3].The paradigm of knee OA is changing from the non-inflammatory “wear and tear” theory to the “low-grade chronic inflammation” hypothesis [4]. In such a case, future treatments should act on the modulation of inflammation to stop/revert OA progression [5].The biomechanical theory states that cartilage overloads because of malalignment, poor biomechanics and impact. Cartilage softens and degrades and subchondral bone stiffens. Afterwards, osteophytes appear to counteract bone destruction and finally the joint breaks down [5]. The inflammatory theory states that cartilage breaks down and apoptosis releases inflammatory cytokines that activate second messengers, perpetuating inflammation, loading to a catabolic state, producing greater cartilage destruction [5].The inflammatory process is supported by inflammatory cytokines released by chondrocytes (IL-1, IL-6, IL-8, IL-17, LIF, TNF-α, IFN-γ) which cooperate in continued cartilage destruction [6]. From all those pro-inflammatory cytokines, IL-1β and TNF-α play a crucial role in the initiation and development of OA [4]. IL-1 is responsible for cartilage destruction while TNF-α activates the inflammatory process [4]. Both IL-1β and TNF-α induce chondrocytes and synovial cells in the production of other pro-inflammatory cells, such as IL-6 [4]. IL-1 affects the production of Reactive Oxygen Species (ROS) which are implicated in the damage of the DNA of chondrocytes [6]. ROS accelerate cartilage matrix disintegration and joint space narrowing, inhibiting synthesis of proteoglycans and collagen [6]. IL-6 increases the number of inflammatory cells in synovial tissue, stimulating the proliferation of chondrocytes and amplification of IL-1β effect [4]. Inflammatory cytokines stimulate proteolytic enzymes such as metalloproteinases (MMPs), leukemia inhibitor factor (LIF) and Oncostatin M (OSM) to enhance degradation of cartilage and apoptosis [5,6].Based on the previous assumptions, the future therapy on knee OA should inhibit pro-inflammatory cytokines (IL-1β, TNF-α, IL-6), proteolytic enzymes (MMPs), NOS (nitric oxide synthase) and apoptosis. On the other hand, OA management should stimulate the synthesis of anti-inflammatory cytokines (IL-4, IL-10, IL-13) and growth factors (TGF-β, IGF-1, and so forth) [4]. There must be a balance in favor of anabolic/anti-inflammatory factors, reducing catabolic/pro inflammatory factors (Figure 1) [3,5].
Figure 1. Osteoarthritis is the result of an imbalance between anabolic and catabolic factors where pro-inflammatory cytokines and catabolic chemokines predominates over anti-inflammatory cytokines and anabolic chemokines (Fernandez-Cuadros et al. [5]). Legend: MMP, matrix mineral metalloproteases. ADAMs, disintegrin and metalloprotease. ADAMTS, disintegrin and metalloprotease with thrombospondin motifs. NO, nitric oxide. TNF-α, tumor necrosis factor α; iNOS, Inducible Nitric Oxide Synthase. COX-2, cyclooxygenase-2. CXCL, chemokine receptor. CCL, chemokine ligand. CRP, C-reactive protein. ESR, erythrocyte sedimentation rate. TGF-β, transforming growth factor β. HGF, hepatocyte growth factor. VEGF, vascular endothelial growth factor. EGF, endothelial growth factor. IGF-1, insulin growing factor 1. HDGF, hepatocyte derived growth factor. TIMPS, Tissue inhibitor of metalloprotease. NF-Kβ, nuclear factor Kβ.IGF-1 (Insulin-like growth factor 1) is an endocrine and autocrine/paracrine growth factor that circulates in plasma at high levels, and it is expressed by most cell types. IGF-1 has major effects on development, cell growth, differentiation and tissue repair [7]. IGF-1 could also block inflammation, oxidative stress and endothelial dysfunction. Therefore, IGF-1 may show anti-inflammatory and pro-repair mechanisms [7].Ozone (O3) is the allotropic or unstable form of oxygen and it is a strong antioxidant after fluorine and persulphate. O3 oxidative properties act as an important anti-infectious, anti-parasitic, anti-viral and anti-fungal agent. O3 dissolved in plasma reacts with several biomolecules generating second messengers such as ROS and LOPs (Lipid Oxidative products), which are finally responsible for the biological and therapeutical effects. Therefore, O3 may exert anti-inflammatory, immunomodulatory and anabolic effects [3].Several studies and many years of clinical experience state that Ozone has proven effects on the modulation of inflammation and in the release of stem cells and growth factors, promoting cartilage growth and joint repair mechanisms [3,6]. A recent review states that O3 can act on the pathogenesis of OA reducing inflammatory cytokines (IL-1β, TNF-α, IFN-γ, C-reactive protein [CRP], erythrocyte sedimentation rate [ESR] and uric acid), reducing catabolic chemokines (MMP, NO), stimulating anti-inflammatory cytokines (IL-4, IL-10, IL-13) and stimulating anabolic chemokines (TGF-β and IGF-1) [5]. Ozone has also been observed to decrease NF-Kβ pathway (inflammatory pathway) and O3 improved Nrf2 pathway, which is involved in the generation of antioxidant response elements (AREs) such as superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx) and hemoxygenase-1(HO-1) [8].Finally, it has been observed that O3 is capable of inhibiting prostaglandins/bradykinin; as a result, reduction of pain and edema were observed. Ozone is also able to stimulate chondrocytes and fibroblasts proliferation; synthesis of articular cartilage and repair of tissue defects are the expected results [6].OA produces a great impact on pain, function and use of health resources. The goals of treatment should try to ameliorate symptoms and to diminish articular damage [3]. Many physicians worldwide use O3 by intra-articular infiltrations to alleviate symptoms of chronic knee OA, such as pain, loss of function and quality of life [3,4,5,6]. However, very few studies have evaluated O3 effect on biomarkers of inflammation and on its reparative/anabolic effect [4], and most of the studies are based on animal models rather than on human patients [3].The objective of the study is: (a) to demonstrate the anti-inflammatory and anabolic effect of Ozone by determining in serum samples the biochemical levels of IL-6 and IGF-1 in knee OA patients in a real world rehabilitation setting; (b) to differentiate Ozone effect in diabetic (DM)/obese and non-DM/non-obese patients; (c) to evaluate clinical effectiveness by visual analog scale (VAS) and WOMAC scale, and biochemical effect by C-reactive protein (CRP), uric acid and erythrocyte sedimentation rate (ESR).
2. Material and Methods
[rml_read_more]; (b) uric acid, (c) erythrocyte sedimentation rate [ESR]; (d) pain (VAS); (e) WOMAC pain, WOMAC stiffness and WOMAC function.Ozone protocol consisted of four sessions (once a week) of an intra-articular infiltration of 20 mL (20 µg/mL concentration) of a gas mixture of Oxygen-Ozone 95-5%. Knee skin was thoroughly cleansed with 1% chlorhexidine and ethyl chloride was used after cleansing as topical anesthetic. A silicone coated syringe of 20 mL was applied to Ozonosan-α plus® (Ozone generator) to get the desired concentration. A 27G Quincke needle of 4 cm was used to infiltrate Ozone into the joint. Ozone was infiltrated on the superior peripatellar pouch with the knee semi flexed. Before the first infiltration and after the fourth infiltration, a venous extraction of 10 mL was performed in order to analyze the biomarkers IL-6 and IGF-1.For IL-6 evaluation, SNIBE MAGLUMI ™ IL-6 (CLIA) kit was used. This kit is a chemoluminiscent immunoassay (CLIA) for quantitative determination of IL-6 in human serum and plasma. For IGF-1 evaluation, the SNIBE MAGLUMI ™ IGF-1 (CLIA) kit was used. This kit is a chemoluminiscent immunoassay (CLIA) for quantitative determination of IGF-1 in human serum and plasma. CRP was analyzed by Abbott Alinity c kit, uric acid was analyzed by Abbott Alinity c kit; and ESR was evaluated by DIESSE VES MATIC CUBE 30.Statistical analysis was performed using SPSS® version 20.0. Means and standard deviation were used for quantitative variables. For a before-and-after evaluation of biochemical markers, T-student was the reference test. Level of significance was established at 95% (p < 0.05).
3. Results
A total of 65 patients were analyzed, 51 non-DM/non-obese knee OA patients, and 14 patients with knee OA, DM and obesity (BMI > 30) were included in the study.There is a linear correlation between age and OA severity, older patients show greater knee OA KL severity. The incidence was greater on mild cases (Table 1).Table 1. Age and outcome variables (IGF-1 and IL-6) before-and after treatment, according to osteoarthritis (OA) Kellgren-Lawrence (KL) grades, and if diabetic and obese patients were included or not.
Table 1. Age and outcome variables (IGF-1 and IL-6) before-and after treatment, according to osteoarthritis (OA) Kellgren-Lawrence (KL) grades, and if diabetic and obese patients were included or not.
| Analyzed Groups | AGE Years | IL-6 Pre pg/mL | IL-6 Post pg/mL | p | IGF-1 Pre ng/mL | IGF-1 Post ng/mL | p |
|---|---|---|---|---|---|---|---|
| OA all patients (n = 65) | 67 | 2.07 ± 2.8 | 1.59 ± 1.83 | 0.0684 | 112.09 ± 40.96 | 107.19 ± 36.04 | 0.0299 * |
| OA KL 2° (n = 36) | 62 | 2.19 ± 3.33 | 1.57 ± 1.76 | 117.06 ± 48.67 | 111.91 ± 41.29 | ||
| OA KL 3° (n = 21) | 71 | 2.43 ± 2.55 | 1.99 ± 2.29 | 93.2 ± 23.12 | 93.28 ± 25.01 | ||
| OA KL 4° (n = 8) | 76 | 0.63 ± 0.23 | 0.65 ± 0.43 | 139.3 ± 24.34 | 122.46 ± 28.38 | ||
| OA without DM/obesity (n = 51) | 68.09 | 2.35 ± 3.07 | 1.75 ± 1.94 | 0.0697 | 100.17 ± 28.63 | 102.03 ± 30.67 | 0.2198 |
| OA KL 2° (n = 28) | 63.92 | 2.44 ± 3.51 | 1.64 ± 1.72 | 102.34 ± 31.25 | 104.86 ± 33.59 | ||
| OA KL 3° (n = 19) | 72 | 2.60 ± 2.63 | 2.10 ±2.38 | 90.51 ± 22.16 | 9270 ± 25.59 | ||
| OA KL 4° (n = 4) | 78.75 | 0,5± 0.01 | 0.80 ± 0.60 | 130.85 ± 6.63 | 126.55 ± 12.83 | ||
| OA + DM + obesity (n = 14) | 60.85 | 1.09 ± 0.91 | 1.03 ± 1.23 | 0.8383 | 155.59 ± 50.16 | 125.98 ± 47.87 | 0.0001 * |
| OA KL 2° (n = 8) | 53.87 | 1.31 ± 1.16 | 1.33 ± 1.57 | 168.59 ± 59.23 | 136.58 ± 55.45 | ||
| OA KL 3° (n = 2) | 64.50 | 0.87 ± 0.53 | 0.92 ± 0.59 | 118.75 ± 20.15 | 98.83 ± 25.54 | ||
| OA KL 4° (n = 4) | 73 | 0.76 ± 0.29 | 0.50 ± 0.11 | 147.75 ± 33.88 | 118.37 ± 40.87 |
OA, Osteoarthritis. KL, Kellgren Lawrence. DM, diabetes mellitus. P, T student Test. *, p < 0.05.
IL-6 decreased both in DM and non-DM patients and in all OA KL grades (p = 0.0684). IGF-1 decreased in the total group (OA + DM + obesity), showing that Ozone reduces IGF-1 levels in diabetic patients (p = 0.0299); but, when only knee OA patients are analyzed, O3 improved IGF-1 levels, showing an anabolic effect, as previously observed by some other investigators [3] (Table 1).In 65 OA patients, IL-6 decreased from 2.07 ± 2.8 pg/mL to 1.59 ± 1.83 pg/mL, p = 0.0684 (Table 1). In the same 65 OA patients, IGF-1 decreased from 112.09 ± 40.96 ng/mL to 107.19 ± 36.04 ng/mL, p = 0.0299 (Table 1).However, when obese and DM patients were eliminated, leaving only 51 OA patients without such comorbidities, IGF-1 improved from 100.17 ± 28.63 ng/mL to 102.03 ± 30.67 ng/mL, p = 0.2198 (p > 0.05) (Table 1).In 51 patients, once DM and obesity were excluded, IL-6 decreased from 2.35 ± 3.07 pg/mL to 1.75 ± 1.94 pg/mL, p = 0.0697 (p > 0.05) (Table 1).In 14 DM/obese patients, IL-6 tended to decrease from 1.09 ± 0.91 pg/mL to 1.03 ± 1.23 pg/mL, p = 0.8383 (p > 0.05); and IGF-1 decreased significantly from 155.59 ± 50.16 to 125.98 ± 48.47 ng/mL (p = 0.0001) (Table 1).An overall view reveals that Ozone decreased IL-6 in both DM/obese and non-DM/non-obese knee OA patients. On the contrary, O3 decreased IGF-1 in DM/obese patients (metabolic/hypoglycemic effect), and improved IGF-1 levels in non-DM/non-obese knee OA patients (anabolic effect).When secondary outcomes are evaluated, Ozone decreased C-reactive protein (CRP) [p = 0.0126], erythrocyte sedimentation rate (ESR) [p = 0.0287], and uric acid [p = 0.4436] as biochemical variables. Ozone improved VAS pain, WOMAC pain, WOMAC function and WOMAC stiffness (p < 0.01) as clinical variables in knee osteoarthritis patients (Table 2).
Table 2. Clinical and biochemical variables before-and after Ozone treatment in knee osteoarthritis patients (n = 65).
| Variables | Pre Treatment | Post Treatment | p |
|---|---|---|---|
| Biochemical Variables | |||
| IL-6 pg/mL (mean ± SD) | 2.07 ± 2.80 | 1.59 ± 1.83 | 0.0684 |
| IGF-1 ng/mL (mean ± SD) | 112.09 ± 40.96 | 107.19 ± 36.04 | 0.0299 * |
| CRP mg/mL (mean ± SD) | 0.42 ± 0.47 | 0.32 ± 0.35 | 0.0126 * |
| Uric acid mg/mL (mean ± SD) | 5.12 ± 1.21 | 5.10 ± 1.13 | 0.4436 |
| ESR mm/h (mean ± SD) | 12.35 ± 8.48 | 11.11 ± 8.11 | 0.0287 * |
| Clinical Variables | |||
| VAS pain (0–10) mean ± SD | 6.89 ± 0.93 | 3.87 ± 1.62 | 0.0001 * |
| WOMAC pain (0–20) mean ± SD | 13.83 ± 1.91 | 7.75 ± 3.25 | 0.0001 * |
| WOMAC stiffness (0–8) mean ± SD | 2.71 ± 1.27 | 1.37 ± 1.15 | 0.0001 * |
| WOMAC function (0–68) mean ± SD | 41.60 ± 7.95 | 27.70 ± 9.43 | 0.0001 * |
IL-6, interleukin 6. IGF-1, Insulin like Growing Factor 1. CRP, C-reactive protein. ESR, Erythrocyte Sedimentation Rate. VAS; visual analogical scale. WOMAC; Western Ontario and McMaster Index for Osteoarthritis. P, T student Test. *, p < 0.05.
4. Discussion
To the best of our knowledge, this is the first study that states the anti-inflammatory, metabolic/hypoglycemic and anabolic effect of O3 therapy on knee OA patients, evaluated by IL-6 and IGF-1 biomarkers in a real world rehabilitation setting.Our study group had previously observed that O3 was capable of modulating inflammation by decreasing CRP (C-reactive protein), ESR (erythrocyte sedimentation rate) and uric acid, improving pain and function (evaluated by VAS [visual analog scale] and WOMAC [Western Ontario and McMaster Index for OA]), and O3 was also capable of increasing joint narrowing space [9,10,11,12,13]. Those previous observations were confirmed again in this cohort of knee OA patients (n = 65). Pan et al. have recently stated that there is evidence that proinflammatory cytokines are key mediators in the pathophysiology of OA [14]. Moreover, IL-6, TNF-α and CRP are linked to knee OA progression and to pain in the short term [14]. Therefore, there is a hypothetical possibility to decrease pain and to delay OA progression by acting on inflammation [14]. In this scenario, we intended to confirm the anti-inflammatory/anabolic properties of Ozone by using specific anti-inflammatory (IL-6) and anabolic (IGF-1) cytokines. Our biochemical observations have confirmed our hypothesis. Ozone tended to decrease IL-6 and tended to improve IGF-1, on an overall view, although not significantly (p > 0.05).Moreover, we have observed a paradoxical effect on DM/obese patients, where Ozone decreased IGF-1 levels; while, in non-DM/non-obese patients, we observed that O3 improved IGF-1 levels. We will further discuss these observations in extent.Our interest to evaluate IL-6 was because IL-6 is implicated in the pathophysiology of OA, in cartilage loss and in pain course in knee OA patients [14]. IL-6 levels were associated to cartilage loss in a follow-up period of 2 and 15 years [15,16]; and IL-6 is also related to moderate pain in knee OA patients [14]. However, targeting IL-6 by anti-IL-6 agents such as Tocilizumab has not reduced pain in such patients in 12 weeks follow-up [17]. We hypothesize that the multi-target profile of Ozone could act on several proinflammatory cytokines, included IL-6. We also postulate that Ozone could release growth factors such as IGF-1.OA is the most common degenerative disease in people over 65 years of age. Many pro-inflammatory mediators are elevated in OA such as ROS, NOS, and hydrogen peroxide (H2O2) [18]. Affected knee OA express elevated inflammatory cytokines such as IL-1β, IL-6, TNF-α, which promote catabolism of cartilage and subchondral bone [19]. ROS formed during OA activates NF-κβ pathway (inflammatory pathway) by increasing its translocation into the nuclei and it causes the activation on intracellular inflammatory cytokines such as IL-1β, IL-6, TNF-α and COX-2 which open the apoptotic cascade [18]. Ozone can inhibit apoptosis and degradation of the cartilage matrix by inhibiting the activation of NF-κβ resulting in cell survival [5,8,18].The effect of ozone in decreasing pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) has been observed in several animal models of knee OA, rheumatoid arthritis and in ischemia/reperfusion models, but not in human knee patients. There lies the importance of this study.In a rat model, Xu et al. have stated that Ozone reduced the concentration levels of IL-6, TNF-α, MMP-13 and degradation of collagen [20]. Guo et al. have stated that intra-articular injections of 40 µg/mL of Ozone could attenuate synovitis in rats with collagen induced arthritis by the inhibition of IL-6, TNF-α and VEGF in serum [21]. Valliant has stated that ozone decreased IL-1β, TNF-α mRNA levels and oxidative stress in a rat model of arthritis induced by PG/PS [22]. Leon-Fernández et al. have stated that in human rheumatoid arthritis patients, O3 reduced pain and reactants of acute phase (CRP, ESR). Although these observations were similar to our previous studies on human knee OA [10], no reference was done about inflammatory cytokines (IL-1β, IL-6, TNF-α, etc.) [23]. In another model of rheumatoid arthritis, Chang et al. have observed that O3 decreased the production of pro-inflammatory cytokines IL-1β, IL-6, and TNF-α [24].As a resume, in all models of rheumatoid arthritis, O3 has been able to decrease pro-inflammatory cytokines (IL-1β, IL-6, TNF-α), then the anti-inflammatory effect of ozone was stated, as it was observed in our study; in which, Ozone tended to reduce IL-6.The anti-inflammatory effect of O3 has also been observed, not only in arthritis models, but in ischemia/reperfusion (I/R) models. Zhang et al. have stated that in a chronic constriction injury model of sciatic nerve in rats, intrathecal injection of O3 inhibited pain and decreased IL-1β, IL-6, TNF-α and NF-κβ/p65, alleviating neuropathic pain [25]. Gultekin et al. have observed that O3 decreased TNF-α but not IL-6 in an I/R liver-injury model in rats [26]. Yildiz has observed that O3 ameliorated the expression of TNF-α and IL-6 in a systemic steroid-induced model of retinal injury [27]. Calunga-Fernández et al. have stated that O3 reduced pro-inflammatory IL-6 in a subtotal nephrectomy model in rats [28]. De Souza et al. have reported that O3 decreased IL-6 levels in a model of animal peritonitis by inactivation of bacteria, probably by oxidation [29]. This comes in line with Bette et al. who observed that O3 decreased pro-inflammatory cytokines (IL-1β and TNF-α) and improved survival rate in a peritonitis model in rats [29]. Gürkan et al. have described that Ozone was capable of reducing IL-1β, TNF-α and IL-6 in an experimental model of spine surgery. O3 was similar to Methylprednisolone, but the combination of both (O3 plus Methylprednisolone) was even more effective [30]. Zamora et al. have observed that in a septic model of peritonitis, Ozone plus antibiotics decreased the expression of IL-1β [31]. O3 activates intracellular mechanisms that inhibit IL-1β, the most important pro-inflammatory cytokine [31].Ersoz et al. have stated that O3 decreased oxidative stress and pro-inflammatory cytokines (TNF-α, IL-6) and improved anti-inflammatory IL-10 in an animal model of colon anastomosis in rats [32]. Merhi et al. has described that in an experimental uterine-adhesion model, O3 at 45 µg/mL and at 60 µg/mL decreased TNF-α and IL-6 [33]. In a chronic model of kidney disease, O3 upregulated antioxidant enzymes (SOD, CAT, GPx), O3 downregulated oxidation products (MDA, PCO) and inflammatory cytokines (IL-1β, IL-6, TNF-α and ICAM) [34]. O3 restored impaired antioxidant Nrf2 pathway and downregulated NF-κβ pathway [34], as it was previously reported by Fernández-Cuadros [5]. Chen et al., in another animal model of chronic kidney disease, observed that O3 ameliorated pro-inflammatory cytokines (IL-1β, IL-6, TNF-α and monocyte chemoattractant protein-1 [MCP-1]) [35]. Finally, Isik et al. have reported that in an intestinal-injury model, O3 improved healing by decreasing TNF-α because of its anti-inflammatory effects [36].Until this point, in animal models of rheumatoid arthritis, in experimental models of I/R of the liver, kidney, sciatic nerve and in experimental models of peritonitis, O3 has shown its anti-inflammatory effect by decreasing pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) and by blocking NF-κβ pathway and by improving Nrf2 pathway. This comes in line with our observations that Ozone tended to decrease IL-6 in human knee OA (p = 0.0684). The anti-inflammatory effect of O3 was suggested by a reduction in IL-6 levels.In a previous study we observed that O3 improved the minimal joint space narrowing evaluated by X-rays, so an anabolic effect was attributable to O3 therapy [9,12,13]. In clinical reviews on the effect of Ozone, it is accepted that O3 stimulates anti-inflammatory cytokines (IL-4, IL-10, IL-13) and growth factors (IGF-1, TGF-β) [3,5,6]. The anabolic effect would explain the improvement on joint space in knee OA patients [13]. We hypothesize that Ozone will improve IGF-1 levels, and this growth factor would be responsible of increasing minimal joint space narrowing, as previously observed by our study group [9,12,13].Surprisingly, in our present study, O3 has demonstrated both a paradoxical (metabolic/hypoglycemic) and anabolic effect. In obese/DM patients, O3 downregulated IGF-1 significantly (p = 0.0299); while in non-obese/non-DM patients, O3 tended to improve IGF-1 levels (p = 0.2198). We will try to elucidate why we observed such IGF-1 variations.IGF-1 has pleiotropic effects on health status such as tissue homeostasis, cardiovascular and neural protection, Insulin-like effects, skeletal development, muscle plasticity and tissue repair [37]. IGF-1 regulates normal growth in childhood, and it has an anabolic effect on adults, acting on muscle growth and tissue repair [38].IGF-1 has a fundamental role in prenatal and postnatal development. Circulating IGF-1 is secreted in the liver by the control of growth hormones [7]. IGF-1 and insulin share common activating pathways. Insulin at physiological concentrations activates insulin, but not IGF-1 hybrid receptors [7]. This occurs because insulin and IGF-1 share structural homology; they interact with same membrane receptors with different affinities to mediate a wide range of metabolic and growth promoting functions [39]. In fact, insulin and IGF-1 differ only in six amino acids. For example, Insulin and IGF-1 increase cellular proliferation and migration in human subacromial bursa tissue [40].IGF-1 has anti-inflammatory properties. There is evidence of relation between IL-6 and IGF-1. In fact, low IGF-1 and high levels of IL-6 and TNF-α are related to mortality in elderly patients [7,41]. Although IGF-1 blocks inflammation, oxidative stress and endothelial dysfunction; paradoxically, IGF-1 deficiency has been linked to increased longevity [7,37]. IGF-1 is increased in DM, myocardial infarction and ventricular hypertrophy [42]. Specifically, IGF-1 is upregulated in in type-2 DM and downregulated in type-1 DM. Elevation of IGF-1 is the result of insulin resistance in obese patients. This elevation constitutes a risk factor for vascular deterioration [38]. This would explain why IGF-1 was elevated in obese/DM patients in our present study.ROS enhance insulin signaling. Considering the substantial similarity between IGF-1 and insulin signaling pathways; it is possible that ROS similarly enhance IGF-1 signaling [43]. On the contrary, since O3 reduces ROS and insulin resistance, it is expected that O3 could reduce IGF-1 in DM/obese patients, as it was observed in our study. A metabolic/hypoglycemic effect of O3 was observed in DM/obese knee OA patients.Since a reduction of food intake decreases signaling activity/bioability of insulin or IGF-1 because they are orthologue compounds; it is expected that a reduction of insulin level by Ozone could also reduce non-physiological bases of IGF-1 [7]. This could explain how it was that O3 reduced IGF-1 in obese/DM or insulin resistant patients, as it was observed in our study (from 112.09 to 107.19 ng/mL, p = 0.0299).There are several reports that state that Ozone acts on diabetic models and in diabetic patients. Saleh et al. observed that O3 plus insulin reduced fasting serum glucose and Hb1Ac after four weeks of treatment in diabetic rats. The antidiabetic effect of O3 seems to be associated with the antioxidant properties of O3 [44]. Erken has observed that O3 decreased blood glucose levels in diabetic rats. Ozone showed a hypoglycemic effect [45].Morsy et al. have reported that in a diabetic nephropathy-model in rats, Ozone was as effective as insulin in producing hypoglycemia and reducing Hb1Ac. They state that O3 and insulin reduce Hb1Ac because both exert independently a hypoglycemic effect. Besides the hypoglycemic effect, Ozone efficacy on DM is attributed to the induction of antioxidant enzyme activity and control of their expression. Therefore, O3 and insulin reduced Hb1Ac; they also reduced ROS production and improved antioxidant enzymes [46].Martinez-Sánchez has stated that O3 improved glycemic control in patients with diabetic foot. They state that O3 activates the antioxidant system, influencing in the level of glycaemia. At the end of O3 treatment, glucose level, which was high despite hypoglycemic drugs (because if insulin resistance), decreased within the normal reference range. The antidiabetic effect of O3 seems to be associated to its antioxidant properties, which increase insulin sensitivity. Finally, in diabetic foot, the superiority of O3 compared to antibiotics is due not only to the O3 antimicrobial effect, but also to its capacity to reduce hyperglycemia. Ozone treatment by means of its oxidative preconditioning effect normalizes glucose levels [47].All previous papers have stated that O3 exerts a hypoglycemic or metabolic effect on diabetic models and in diabetic patients. Since insulin and IGF-1 are very similar compounds (orthologue compounds which differ only in six amino acids); it is expected that in DM/obese patients, the O3 effect will correlate with a decreased of IGF-1 in such patients, as it was observed in our study. On the contrary, excluding DM/obese patients, it is expected to observe an anabolic effect induced by O3 administration and to expect an elevation of IGF-1 in non-obese/non-DM patients. This effect was observed in our study in 51 patients.As previously seen, besides the anti-inflammatory effect of O3, Ozone also reduces MMPs which have a catabolic effect on articular cartilage. Ozone increases antioxidant enzymes (SOD, CAT, GPx, HO-1) and stimulates anti-inflammatory cytokines (IL-4, IL-10, IL-13) and secretes anabolic factors such as IGF-1 and TGF-β [3,5,20]. In our study, O3 improved IGF-1 levels in 51 patients with knee OA.IGF-1 and GH (growth hormone) are anabolic and anti-catabolic growth factors [48]. IGF-1 promotes hypertrophy, regeneration, proliferation and differentiation of skeletal muscles. Ustebay et al. have reported that in an experimental soft tissue injury model in rats, O3 improved IGF-1 levels. Moreover, the level of IGF-1 was correlated with motor function [49]. No other study evaluated previously the effect of O3 on any soft tissue injury model and the relation with IGF-1 [49].Kizilkaya et al. have stated that O3 had beneficial effects on Achilles tendon rupture healing in a rat model after histological and biochemical findings [50]. Duman et al. have stated that O3 improved bone regeneration in a femoral defect model in rats. The physiological effect attributed to Ozone is that O3 improved blood circulation, differentiation, angiogenesis and finally fracture healing [51]. Philippou has stated that IGF-1 is important in regeneration, hypertrophy, proliferation and differentiation of skeletal muscles. Therefore, IGF-1 is related to healing of connective and muscular tissue [52]. These facts support the hypothesis to consider IGF-1 as an anabolic cytokine and since in our study, O3 improved levels of IGF-1 in knee OA patients, the anabolic effect of Ozone is elucidated.Finally, Wang et al. state that clinical benefit of O3 in lumbar interbody fusion using a channel system combined with ozone therapy for L3-L4 lumbar disc herniation is that O3 improves IL-10 and IGF-1. Ozone reduces inflammation (by IL-10 reduction) and improves healing (by IGF-1 improvement) [53].The strength of the study is that biochemical changes observed in the study were correlated with the clinical variables. The main limitation of the study is that there is no control group. However, in a before and after study, the effect of an intervention results from a change from baseline to the end of treatment (Ozone treatment). The natural history of knee OA is cartilage degradation, knee pain and loss of function [1]. On the contrary, an improvement of this condition would be expected as a result of Ozone intervention. The catabolic and proinflammatory cytokines are supposed to be modified by Ozone properties. In any case, although it is unethical to deny a beneficial intervention to knee OA patients, a RCT (randomized control trial) would be desirable to prove our present observations.
5. Conclusions
Ozone is a valid option for the management of knee osteoarthritis because of its anti-inflammatory, metabolic and anabolic properties. Ozone tends to decrease the levels of pro-inflammatory IL-6 cytokine. Ozone has a paradoxical (metabolic) effect on obese/diabetic knee osteoarthritis patients by reducing IGF-1. Ozone has an anabolic effect on non-diabetic/non-obese patients by improving IGF-1. Ozone reduces other biomarkers of inflammation (CRP, ESR and uric acid) and improves, pain, function and quality of life.
References
- Fernández-Cuadros, M.E. Ozone Fundamentals and Effectiveness on Knee Pain: Chondromalacia and Knee Osteoarthritis; LAP LAMBERT Academic Publishing: Saarbrücken, Germany, 2016. [Google Scholar]
- Richards, M.M.; Maxwell, J.S.; Weng, L.; Angelos, M.G.; Golzarian, J. Intra-articular treatment of knee osteoarthritis: From anti-inflammatories to products of regenerative medicine. Phys. Sportsmed. 2016, 44, 101–108. [Google Scholar] [CrossRef]
- Fernandez-Cuadros, M.E.; Perez-Moro, O.S.; Mirón-Canelo, J.A. Could ozone be used as a feasible future treatment in osteoarthritis of the knee. Divers. Equal Health Care 2016, 13, 232–239. [Google Scholar] [CrossRef]
- Rankothgedera, S.; Atukorala, I.; Fernando, C.; Munidasa, D.; Wijayaratne, L.; Udagama, P. A potential diagnostic serum immunological marker panel to differentiate between primary and secondary knee osteoarthritis. PLoS ONE 2021, 16, e0257507. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cuadros, M.E.; Pérez-Moro, O.S.; Albaladejo-Florín, M.J.; Álava-Rabasa, S.; Tobar-Izquierdo, M.; Rodriguez-de-Cía, J. A new paradigm for the management of knee osteoarthritis: The role of hyaluronic acid, platelet-rich plasma (PRP) and ozone in the modulation of inflammation: A review. JSR 2020, 1–8. [Google Scholar] [CrossRef]
- Oliviero, A.; Giordano, L.; Maffulli, N. The temporal effect of intra-articular ozone injections on pain in knee osteoarthritis. Br. Med. Bull. 2019, 132, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Higashi, Y.; Sukhanov, S.; Anwar, A.; Shai, S.Y.; Delafontaine, P. Aging, atherosclerosis, and IGF-1. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2012, 67, 626–639. [Google Scholar] [CrossRef]
- Fernández-Cuadros, M.E.; Albaladejo-Florín, M.J.; Peña-Lora, D.; Álava-Rabasa, S.; Pérez-Moro, O.S. Ozone (O3) and SARS-CoV-2: Physiological bases and their therapeutic possibilities according to COVID-19 evolutionary stage. SN Compr. Clin. Med. 2020, 2, 1094–1102. [Google Scholar] [CrossRef]
- Fernández-Cuadros, M.E.; Pérez-Moro, O.; Albaladejo-Florin, M.J.; Álava-Rabasa, S. Intra-articular ozone modulates inflammation, ameliorates pain and rigidity, improves function and has anabolic effect on knee osteoarthritis: A prospective quasi-experimental before-and-after study, 115 patients. Rev. Soc. Esp. Dolor 2020, 27, 78–88. [Google Scholar]
- Fernandez-Cuadros, M.E.; Perez-Moro, O.S.; Albaladejo-Florin, M.J.; Algarra-Lopez, R. Ozone decreases biomarkers of inflamation (C-reactive protein and erytrocyte sedimentation rate) and improves pain, function and quality of life in knee osteoarthrtitis patients: A before-and-after study and review of the literature. Middle East J. Rehabil. Health 2018, 5, e64507. [Google Scholar] [CrossRef]
- Fernandez-Cuadros, M.E.; Perez-Moro, O.S.; Albaladejo-Florin, M.J.; Algarra-Lopez, R. Intra articular ozone reduces serum uric acid and improves pain, function and quality of life in knee osteoarthritis patients: A before-and-after study. Middle East J. Rehabil. Health 2018, 5, e68599. [Google Scholar] [CrossRef]
- Fernandez-Cuadros, M.E.; Susana Perez-Moro, O.; Jesus Albaladejo-Florin, M. Knee osteoarthritis: Condroprotector action and symptomatic effect of ozone on pain, function, quality of life, minimal joint space and knee arthroplasty delay. Middle East J. Rehabil. Health 2017, 4, e43200. [Google Scholar] [CrossRef]
- Fernández-Cuadros, M.E.; Pérez-Moro, O.S.; Albaladejo-Florín, M.J.; Álava-Rabasa, S. Symptomatic (Pain and Inflammation) and Disease-Modifying Effect (Minimal Joint Space) of Intra-articular Ozone (O2-O3) in Osteoarthritis of the Knee: A Clinical Case. SN Compr. Clin. Med. 2019, 1, 817–821. [Google Scholar] [CrossRef]
- Pan, F.; Tian, J.; Cicuttini, F.; Jones, G. Prospective Association Between Inflammatory Markers and Knee Cartilage Volume Loss and Pain Trajectory. Pain Ther. 2021, 1–13. [Google Scholar] [CrossRef]
- Livshits, G.; Zhai, G.; Hart, D.J.; Kato, B.S.; Wang, H.; Williams, F.M.; Spector, T.D. Interleukin-6 is a significant predictor of radiographic knee osteoarthritis: The Chingford study. Arthritis Rheum. 2009, 60, 2037–2045. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, J.P.; Raynauld, J.P.; Caron, J.; Mineau, F.; Abram, F.; Dorais, M.; Haraoui, B.; Choquette, D.; Martel-Pelletier, J. Decrease in serum level of matrix metalloproteinases is predictive of the disease-modifying effect of osteoarthritis drugs assessed by quantitative MRI in patients with knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 2095–2101. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Latourte, A.; Sellam, J.; Wendling, D.; Piperno, M.; Goupille, P.; Pers, Y.-M.; Eymard, F.; Ottaviani, S.; Ornetti, P.; et al. Efficacy of tocilizumab in patients with hand osteoarthritis: Double blind, randomised, placebo-controlled, multicentre trial. Ann. Rheum. Dis. 2021, 80, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Manoto, S.L.; Maepa, M.J.; Motaung, S.K. Medical ozone therapy as a potential treatment modality for regeneration of damaged articular cartilage in osteoarthritis. Saudi J. Biol. Sci. 2018, 25, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Mobasheri, A.; Rayman, M.P.; Gualillo, O.; Sellam, J.; Van Der Kraan, P.; Fearon, U. The role of metabolism in the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2017, 13, 302–311. [Google Scholar] [CrossRef]
- Xu, W.; Zhao, X.; Sun, P.; Zhang, C.; Fu, Z.; Zhou, D. The effect of medical ozone treatment on cartilage chondrocyte autophagy in a rat model of osteoarthritis. Am. J. Transl. Res. 2020, 12, 5967. [Google Scholar]
- Guo, R.; Zhang, G.; Zhang, L.; Liu, N.; Ren, L.; Fan, J.; Hou, J. The effect of intra-articular ozone injection on the cytokines of collagen-induced arthritis. Chin. J. Rheumatol. 2017, 21, 247–251. [Google Scholar]
- Vaillant, J.D.; Fraga, A.; Díaz, M.T.; Mallok, A.; Viebahn-Hänsler, R.; Fahmy, Z.; Barbera, A.; Delgado, L.; Menendez, S.; Fernández, O.S.L. Ozone oxidative postconditioning ameliorates joint damage and decreases pro-inflammatory cytokine levels and oxidative stress in PG/PS-induced arthritis in rats. Eur. J. Pharmacol. 2013, 714, 318–324. [Google Scholar] [CrossRef]
- Fernández, O.S.L.; Viebahn-Haensler, R.; Cabreja, G.L.; Espinosa, I.S.; Matos, Y.H.; Roche, L.D.; Santos, B.T.; Our, G.T.; Vega, J.C.P. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 2016, 789, 313–318. [Google Scholar] [CrossRef]
- Chang, J.D.; Lu, H.S.; Chang, Y.F.; Wang, D. Ameliorative effect of ozone on cytokine production in mice injected with human rheumatoid arthritis synovial fibroblast cells. Rheumatol. Int. 2005, 26, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, F.; Zhang, L.; Sun, T.; Fu, Z. Intrathecal injection of ozone alleviates CCI-induced neuropathic pain via the GluR6-NF-κB/p65 signalling pathway in rats. Mol. Med. Rep. 2021, 23, 231. [Google Scholar] [CrossRef] [PubMed]
- Gultekin, F.A.; Cakmak, G.K.; Turkcu, U.O.; Yurdakan, G.; Demir, F.E.O.; Comert, M. Effects of ozone oxidative preconditioning on liver regeneration after partial hepatectomy in rats. J. Investig. Surg. 2013, 26, 242–252. [Google Scholar] [CrossRef]
- Yıldız, A.; Şehitoğlu, M.H.; Karaboğa, İ.; Arıkan, S. Ozone treatment for high-dose systemic Steroid-Induced retinal injury. Cutan. Ocul. Toxicol. 2020, 39, 274–280. [Google Scholar] [CrossRef]
- Calunga, J.L.; Zamora, Z.B.; Borrego, A.; Río, S.D.; Barber, E.; Menéndez, S.; Taboada, D. Ozone therapy on rats submitted to subtotal nephrectomy: Role of antioxidant system. Mediat. Inflamm. 2005, 2005, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Souza, Y.M.D.; Fontes, B.; Martins, J.O.; Sannomiya, P.; Brito, G.S.; Younes, R.N.; Rasslan, S. Evaluation of the effects of ozone therapy in the treatment of intra-abdominal infection in rats. Clinics 2010, 65, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Gürkan, G.; Sayin, M.; Kizmazoglu, C.; Erdogan, M.A.; Yigitturk, G.; Yilmaz, H.E.; Uzunoglu, I.; Kaya, I.; Yuceer, N. Evaluation of the neuroprotective effects of ozone in an experimental spine injury model. J. Neurosurg. 2020, 33, 406–414. [Google Scholar] [CrossRef]
- Zamora, Z.B.; Menéndez, S.; Bette, M.; Mutters, R.; Hoffmann, S.; Schulz, S. Ozone Prophylactic Effect and Antibiotics as a Modulator of Inflamatory Septic process in Rats. In Proceedings of the 16th International Ozone Association World Congress, Las Vegas, NV, USA, 31 August–5 September 2003; p. 123. [Google Scholar]
- Ersoz, N.; Ozler, M.; Topal, T.; Uysal, B.; Poyrazoglu, Y.; Simsek, K.; Gocgeldi, E.; Korkmaz, A. The effect of ozone treatment on experimental colon anastomosis in rats. Eur. Surg. 2016, 48, 122–128. [Google Scholar] [CrossRef]
- Merhi, Z.; Garg, B.; Moseley-LaRue, R.; Moseley, A.R.; Smith, A.H.; Zhang, J. Ozone therapy: A potential therapeutic adjunct for improving female reproductive health. Med. Gas Res. 2019, 9, 101. [Google Scholar] [CrossRef]
- Yu, G.; Liu, X.; Chen, Z.; Chen, H.; Wang, L.; Wang, Z.; Qiu, T.; Weng, X. Ozone therapy could attenuate tubulointerstitial injury in adenine-induced CKD rats by mediating Nrf2 and NF-κB. Iran. J. Basic Med. Sci. 2016, 19, 1136. [Google Scholar]
- Chen, Z.; Liu, X.; Yu, G.; Chen, H.; Wang, L.; Wang, Z.; Qiu, T.; Weng, X. Ozone therapy ameliorates tubulointerstitial inflammation by regulating TLR4 in adenine-induced CKD rats. Ren. Fail. 2016, 38, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Isik, A.; Peker, K.; Gursul, C.; Sayar, I.; Firat, D.; Yilmaz, I.; Demiryilmaz, I. The effect of ozone and naringin on intestinal ischemia/reperfusion injury in an experimental model. Int. J. Surg. 2015, 21, 38–44. [Google Scholar] [CrossRef]
- Vitale, G.; Pellegrino, G.; Vollery, M.; Hofland, L.J. ROLE of IGF-1 system in the modulation of longevity: Controversies and new insights from a centenarians’ perspective. Front. Endocrinol. 2019, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Bailes, J.; Soloviev, M. Insulin-Like Growth Factor-1 (IGF-1) and Its Monitoring in Medical Diagnostic and in Sports. Biomolecules 2021, 11, 217. [Google Scholar] [CrossRef] [PubMed]
- Kuang, J.; Zhang, L.; Xu, Y.; Xue, J.; Liang, S. Association between insulin-like growth factor 1 and insulin resistance in obese prepubertal boys: A cross-sectional study. Res. Sq. 2020, 1–10. [Google Scholar] [CrossRef]
- Muench, L.N.; Tamburini, L.; Kriscenski, D.; Landry, A.; Berthold, D.P.; Kia, C.; Cote, M.P.; McCarthy, M.B.; Mazzocca, A.D. The Effect of Insulin and Insulin-like Growth Factor 1 (IGF-1) on Cellular Proliferation and Migration of Human Subacromial Bursa Tissue. Arthrosc. Sports Med. Rehabil. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Roubenoff, R.; Parise, H.; Payette, H.A.; Abad, L.W.; D’Agostino, R.; Jacques, P.F.; Wilson, P.W.F.; Dinarello, C.A.; Harris, T.B. Cytokines, insulin-like growth factor 1, sarcopenia, and mortality in very old community-dwelling men and women: The Framingham Heart Study. Am. J. Med. 2003, 115, 429–435. [Google Scholar] [CrossRef]
- Bleumink, G.S.; Schut, A.F.C.; Sturkenboom, M.C.J.M.; Janssen, J.A.M.J.L.; Witteman, J.C.M.; Van Duijn, C.M.; Hofman, A.; Stricker, B.C. A promoter polymorphism of the insulin-like growth factor-I gene is associated with left ventricular hypertrophy. Heart 2005, 91, 239–240. [Google Scholar] [CrossRef]
- Loh, K.; Deng, H.; Fukushima, A.; Cai, X.; Boivin, B.; Galic, S.; Bruce, C.; Shields, B.J.; Skiba, B.; Ooms, L.M.; et al. Reactive oxygen species enhance insulin sensitivity. Cell Metab. 2009, 10, 260–272. [Google Scholar] [CrossRef]
- Saleh, S.; El-Ridi, M.; Zalat, S.; El-Kotb, S.; Donia, S. Additive effect of ozone therapy to insulin in the treatment of diabetic rats. Menoufia Med. J. 2014, 27, 85. [Google Scholar]
- Erken, H.A.; Genc, O.; Erken, G.; Ayada, C.; Gündoğdu, G.; Doğan, H. Ozone partially prevents diabetic neuropathy in rats. Exp. Clin. Endocrinol. Diabetes 2015, 123, 101–105. [Google Scholar] [CrossRef]
- Morsy, M.D.; Hassan, W.N.; Zalat, S.I. Improvement of renal oxidative stress markers after ozone administration in diabetic nephropathy in rats. Diabetol. Metab. Syndr. 2010, 2, 1–7. [Google Scholar] [CrossRef]
- Martínez-Sánchez, G.; Al-Dalain, S.M.; Menéndez, S.; Re, L.; Giuliani, A.; Candelario-Jalil, E.; Álvarez, H.; Fernández-Montequín, J.I.; León, O.S. Therapeutic efficacy of ozone in patients with diabetic foot. Eur. J. Pharmacol. 2005, 523, 151–161. [Google Scholar] [CrossRef]
- Mohammadjafari, H.; Arazi, H.; Nemati, N.; Bagherpoor, T.; Suzuki, K. Acute Effects of Resistance Exercise and the Use of GH or IGF-1 Hormones on Oxidative Stress and Antioxidant Markers in Bodybuilders. Antioxidants 2019, 8, 587. [Google Scholar] [CrossRef]
- Üstebay, S.; Özturk, Ö.; Bilge, A.L.İ.; Üstebay, D.Ü.; Tezcan, A.H. Impacts of ozone treatment and its relationship with IGF-1 levels after injury of soft tissue: An experimental study in rats model. Kafkas Üniv. Vet. Fakültesi Dergisi 2017, 23, 967–971. [Google Scholar] [CrossRef]
- Kizilkaya, V.; Uruc, V.; Levent, A.; Kanat, O.; Yildizgoren, M.T.; Dogramaci, Y.; Kalaci, A. Effectiveness of Ozone Therapy on Tendon Healing: An Experimental Study in Generated Achilles Tendon Injury Model in Rats. J. Hard Tissue Biol. 2018, 27, 309–314. [Google Scholar] [CrossRef]
- Duman, I.G.; Davul, S.; Gokce, H.; Gonenci, R.; Özden, R.; Uruc, V. Effects of gaseous ozone treatment on bone regeneration in femoral defect model in rats. J. Hard Tissue Biol. 2017, 26, 7–12. [Google Scholar] [CrossRef]
- Philippou, A.; Maridaki, M.; Halapas, A.; Koutsilieris, M. The role of the insulin-like growth factor 1 (IGF-1) in skeletal muscle physiology. In Vivo 2007, 21, 45–54. [Google Scholar] [PubMed]
- Wang, Y.; Sun, H.; Qin, S. Clinical efficacy of lumbar interbody fusion using a channel system combined with ozone therapy for the treatment of central-type L3-L4 lumbar disc herniation. Exp. Ther. Med. 2017, 13, 619–623. [Google Scholar] [CrossRef] [PubMed]
